$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Golden Month Professional Coach 11 Transform Your Postnatal Care Vision – Become a Certified Golden Month Coach Revolutionize Maternal Support – Discover Our Online Training to Be... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Baby Sleep Coach 16 Transform Children's Sleep – Become a Certified Baby Sleep Coach. Redefine Your Vision of Family Well-Being – Discover Our Training to Become a... Take this Course
Free Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course in Narcissist Recovery 1466 Free the Bound Souls – Become a Certified Post-Narcissistic Healing Expert. Transform Your Understanding of Narcissistic Abuse – Discover Our Co...
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course in Atlantean Dolphin Reiki 1226 Awaken Your Atlantean Healing Power – Become a Master in Atlantean Dolphin Reiki. Dive into the depths of ancestral energy wisdom – Discover our... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Human Design Coach 1801 Unveil the Energetic Essence of Beings – Become an Expert in Human Design. Unlock the Mysteries of the Human Energy Code – Discover Our Comprehe... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Muslim Coach 1199 Elevate Your Calling – Become a Certified Muslim Coach. Transform lives through guidance that unifies professional excellence and Islamic wisdom... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Birth Doula 1249 Become the Sacred Ally of Birth – Certified Birth Doula Training. Revolutionize Birth Support – Discover Our Excellence Training to Become a Cer... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Moon Cycle Ritual Facilitator 1352 Become a Lunar Cycle Ritual Facilitator – A Sacred Path of Feminine Support. Unveil the mysteries of the menstrual cycle and guide women towards... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Sexual Mindfulness Practitioner 1281 Transform Your Vision of Sexuality – Become a Certified Practitioner in Sexual Mindfulness. Push the Boundaries of Sexological Support – Discove... Take this Course
Free Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Conscious Kink Educator 1418 Reveal the Art of Conscious Kinky Education – Become a Certified Conscious Kink Educator. Transcend the Boundaries of Conventional Sexuality – D...
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Sacred Masculine & Feminine Tantra Practitioner 1271 Awaken the Wisdom of Sacred Tantra – Become a Certified Practitioner of Sacred Masculine & Feminine Tantra. Transcend the Limits of Ordinary... Take this Course
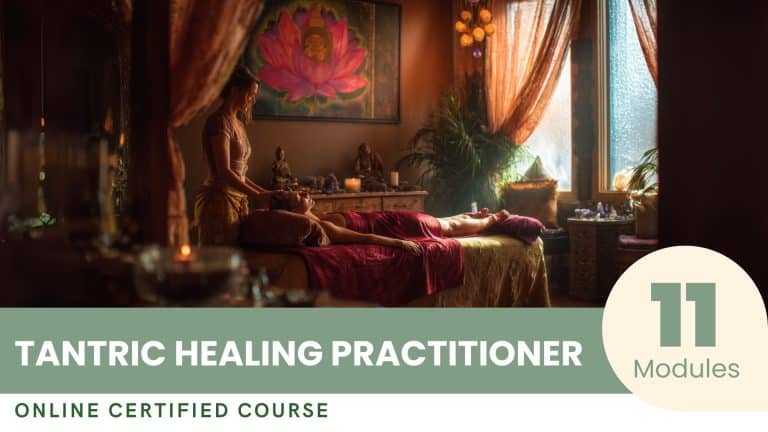
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Tantric Healing Practitioner 1308 Awaken the Tantric Healer Within You – Become a Certified Practitioner in Tantric Healing. Transcend the Boundaries of Traditional Healing – Dis... Take this Course
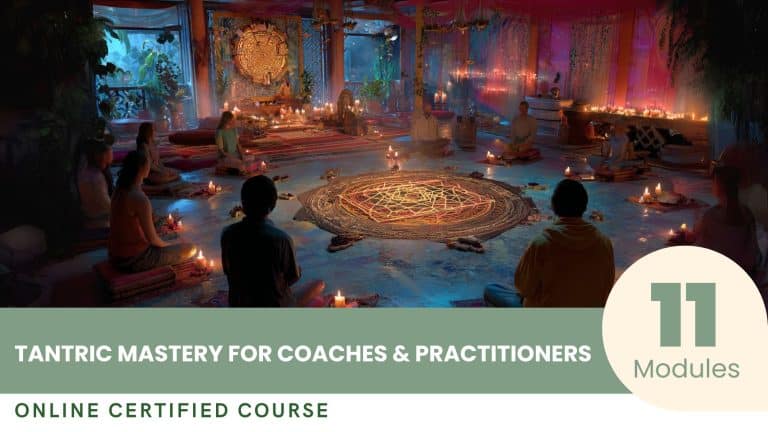
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Tantric Mastery for Coaches & Practitioners 1267 Awaken Tantric Mastery – Become a Certified Coach & Practitioner in Tantrism. Transcend the Limits of Traditional Coaching – Discover Our Ex... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Karmic Realignment Practitioner 1266 Unveil Your Divine Mission – Become a Certified Practitioner in Karmic Realignment. Transcend the Limits of Human Consciousness – Discover Our E... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Women’s Circle Facilitator 1653 Awaken the Sacred Circle – Become a Certified Women's Circle Facilitator. Awaken the ancestral art of women's facilitation – Discover our Profes... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Fertility Coach 1338 Transform Hope into Reality – Become a Certified Fertility Coach. Explore the Sacred Art of Fertility Coaching – Discover Our Excellence Program... Take this Course
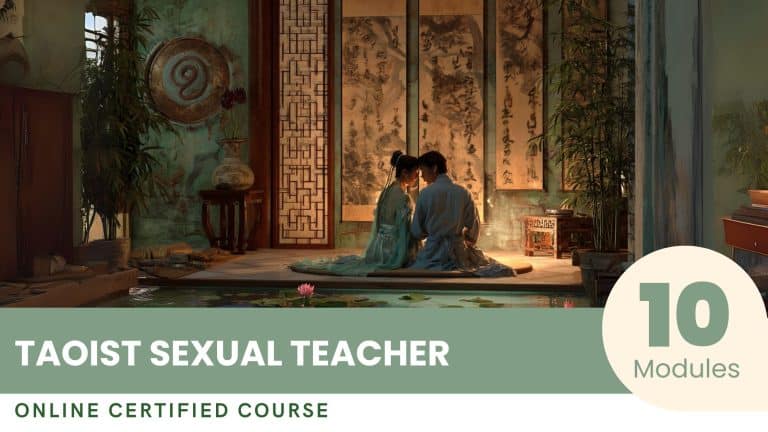
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Taoist Sexual Teacher 1319 Master the Sacred Art of Taoist Sexuality – Become a Certified Teacher. Transcend the Limits of Sexual Guidance – Discover Our Excellence Traini... Take this Course
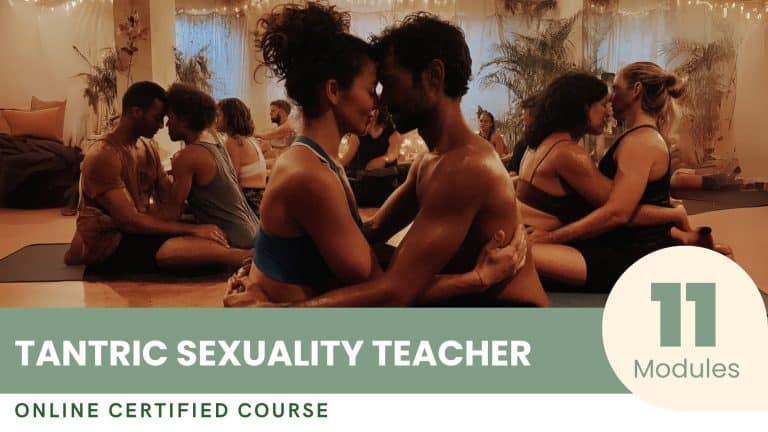
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Tantric Sexuality Teacher 2342 Awaken the Sacred Art of Sexuality – Become a Certified Tantric Sexuality Teacher. Transcend Conventional Boundaries of Guidance – Discover Our... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Retreat Organizer 1594 Become a Creator of Transformational Experiences – The Certification of Excellence in Retreat Organization. Master the sacred art of designing a... Take this Course
$90 Get Now Add To Cart $247.00 Original price was: $247.00.$62.00Current price is: $62.00. By Certified Excellence Team Certified Course to Become a Yoga Event Manager 1212 Orchestrate the Harmony of Yoga – Become a Certified Yoga Event Manager. Transform your passion for yoga into a creative and inspiring event man... Take this Course